
First a mea culpa, I have a huge backlog of relatively heavy articles that I really want to add to the blog. But I’ve been busy getting married – congratulations to me – and I didn’t have enough time. I strongly believe in following relatively strict guidelines on writing and editing articles, where I set myself deadlines and avoid over-writing on topics – it is just a blog after all – but for deep insights I do also have a minimum standard that I want to be able to produce before I’m willing to hit the Publish button.
In keeping with my blog publishing policy, I instinctively follow a similar path in projects. At some point in recent years, I read the book Designing Your Life and discovered that I was following a very similar process to the one which they describe. A similar process is described, perhaps slightly less systematically, in Cal Newport‘s book So Good They Can’t Ignore You.
Essentially I follow a path of Build, Test/Learn and Move. I think this has also been popularised under the term Small Bets. I choose a direction. I build something in that direction. I then test or evaluate my progress. This can encompass many aspects, from my technical fit to the project to inter-personal issues which arose and from which I can learn. I make a lot of notes as I go, to facilitate this process. I try to incorporate any important learnings from the experiment, usually by noting them in a long-term notebook which I review at regular intervals. And then I move on to the next thing. Sometimes the next thing is a continuation of the last thing. What is important is that, each cycle involves a distinct end point even if I do subsequently go further in that direction.
I drew this image about two months ago
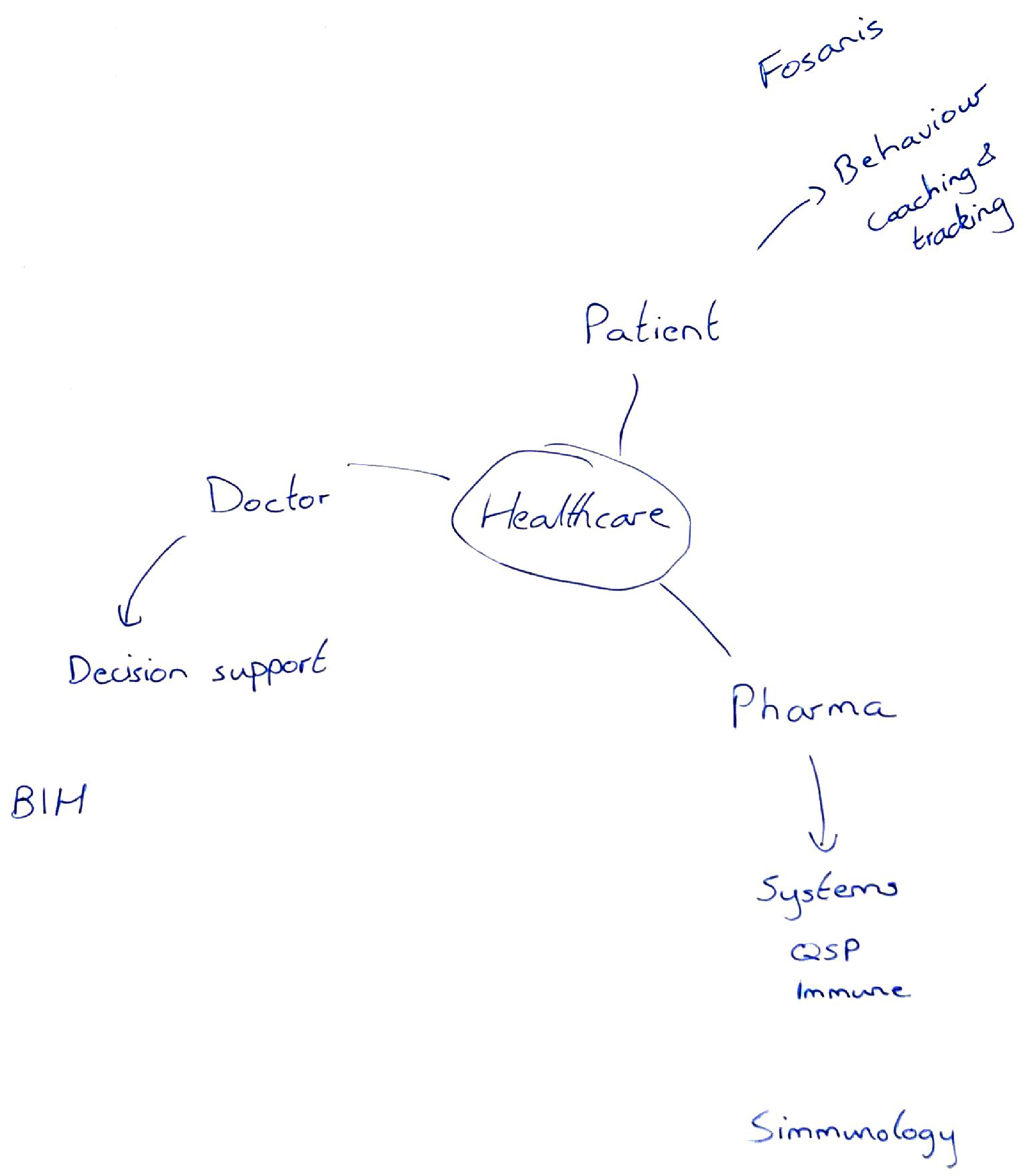
It’s a mind map of my projects over the past 2 years.
I set myself the goal of exploring projects in healthcare when I left academia. I had a lot of doors open to me, but I didn’t know which one I wanted to walk through. I was pretty sure I wanted to leave a pure academic track, but I was afraid of making decisions which would lock me in for the rest of my life. In addition, I was limiting myself to positions in Berlin which actually lacks any real tech/healthcare jobs [I know it’s not what you read in the newspapers. Buy me a coffee and I’ll happily explain.]
As I see it, if you want to deliver solutions in healthcare you have three major branches on which you can work. Most people are, of course, restricted by their skillset, but as a mathematical technologist living in 2019 I can work in all three.
Pharma / Drug development
If you want to impact on patients, one of the greatest points of impact is to work in the pharmaceutical industry. Ultimately, drugs cure people. The main point of working in the pharma sector is to develop new drugs and impact on human health.
[Aside] You can read as many conspiracy theories as you like about profiteering in the industry. The truth is, every credible study has shown that the industry has been largely unprofitable since 2005. In 2018 the sector finally turned a profit. The question for the future is whether this is, like the occasional colder winter since climate change has accelerated, an example of increased variance or is it the restoration of long term profitability. [/Aside]
With this in mind. I started my company Simmunology in early 2018. I had an insight, that drug development is too focused on the point at which symptoms appear and are missing the systemic causes of modern illnesses. With complex adaptive systems, it is preferable to attack the root cause, if possible, rather than maintain a deteriorating orbit on a non-viable complex attractor [a topic I worked on for a year in 2009].
There was no company, at the time, where I could work on my idea. So I looked for a cofounder, looked for funding, and started my own. In the process of finding funding, we acquired a very impressive advisory panel all of whom believed in our idea and in our ability to deliver on it. We also found a number of potential customers who were willing to work on a pilot study together.
We raised enough funding to survive for roughly a year. We were also, in the process of raising a VC round which would have allowed us to hire a team. At this point, some problems became impossible to ignore and I pulled the plug on the entire enterprise. This was unfortunate, as it was my favourite idea to work on. But part of my process is not to get stuck on favourites which are not going to work out. We had problems on the founding team and these predicted badly for our ability to execute.
Patient
An alternative to developing new drugs is to find other ways to help the patient. Some startups provide solutions to managing medical appointments. I was a bit more ambitious, you could say I wanted a digital pill.
A number of years ago I sketched out an idea for delivering behavioural interventions via digital means. My idea was to target neglected patient populations, suffering from autoimmune diseases. These population groups cluster in rich western countries and are typically highly active on niche online fora. I wanted to leverage their goodwill to build a ‘nudging’ tool from the bottom up.
On a technical level, I realised that training data models for medicine is always a fight against low sample size (N). However, we can bootstrap the process by using expert knowledge to do more targetted sampling. I wanted to build a platform on which the community could suggest their own nudges. I would then build them into an App. And we would use A/B testing of the algorithms (and the individual nudges) to test what actually works. Over time, this should lead to true insights which can be mechanically built into algorithms and – fingers crossed – a higher quality exploration of nudge-space which might improve the signal-to-noise ratio for training a machine learning implementation.
In parallel to setting up Simmunology, I had shared this idea with the founders at Fosanis. I helped them to write an industrial research grant proposal using this idea to deliver psychological support to cancer patients. When Simmunology shut down, they convinced me to join them and deliver on the proposal.
While at Fosanis, I hired roughly 14 people most of whom were technical experts (devs, ML engs.). I led my own team of 5 data scientists. I supervised the wider tech team. And I was the person most responsible for keeping the team focused on Product progress. I got to work on the harder parts of software design (e.g. ask me about using Python decorators to do A/B testing!) but I wrote very little code myself 🙁
After a year, I decided to leave Fosanis. I had delivered on the pipeline. The entire infrastructure was in place. It was becomming a question of waiting for the expanded Content and Product teams to catch-up. I decided my time was better spent elsewhere.
I learned an enormous amount about team management while at Fosanis. The biggest team which I have managed to date was 20 people, but a start-up is much more intense! More importantly, I gained the insights I needed as to how and to what degree it is possible to build the type of product which I really wanted to produce. It is bloody hard, but it is possible. Team is everything in this kind of venture.
Doctor
Finally, the other major point at which you can impact on healthcare, using technical means, is by aiding the doctor. In practice, the current trend is towards Decision Support Systems.
By a curious coincidence – or was it hard work on my part – I have been involved with the Berlin Institute of Health since early 2018. They are responsible for translational research and technology transfer for both the Charité Hospital and the Max-Delbrueck Center in Berlin. I was the inaugural keynote, at their rebranded Digital Health Forum in March 2018, speaking about AI in Healthcare.
Over the course of almost two years, we have built a high level of mutual trust where they can rely on me to provide senior expertise in questions on data handling, modelling of health data, and appropriate use of ML approaches. As a mentor, I have had the priviledge of gaining an overview of most of the projects in the first three years of their incubator.
Working with potential spin-outs has allowed me to place a large number of small bets. So far, I have focused most of my energies on two projects developing clinical decision support systems – one using images, and the other using electronic health records – in very different domains. It has been particularly enjoyable to scale my knowledge across a wide number of projects, in this domain, rather than getting stuck in a single technical approach.
My biggest learning from this sector is that electronic health records are going to be a very interesting challenge to crack. Conceptually, they resemble time series. However, they are (i) massively discontinuous, (ii) lacking follow-up, and (iii) contain sparse-diversity in their dimensions. This is a nightmare. However, it is also the most fun!
Dealing with early-stage startups there are limitations on how far I can push their technology. What I really want to do in this space is to take inspiration from financial modelling and build a family of models for the eHR. More on this later.
What next?
Three projects, in the three branches of healthcare. What did I learn?
- I love working on mathematical modelling and algorithms for healthcare.
- I can manage a team. I’m actually pretty good at it.
- I probably won’t be happy doing only management at this point in my career. I love the technical questions too much.
- Architecting systems is probably enough to solve my apetite for technical work. I am supremely good at architecting such systems.
I don’t see myself going back to the nudging project any time soon. It requires the type of team which only seems to exist in companies like Apple.
I am currently working on a short-term bet in another direction. It is a continuation of something which I was working on, during my final postdoc, on causal inference. It could lead in a direction of general AI, or it could as easily lead towards a nice advanced methods project in pharma.
Roll on 2020.
Addendum
My list of areas through which I could impact on healthcare is of course not exhaustive. I want to give an honourable shoutout to mTomady who I met last week. Empowering access to healthcare is a truly noble application.